
THE VACCINES ARE NOT SAFE
YOU MUST WATCH THIS VIDEO
What we Observe in the JABS
Adverse Effects Continue
Former Pfizer Employee Whistleblower Tells How Dangerous These JABS Really Are
More Physicians are testifying to the problems inherent in the way the SARS-CoV-2 vaccines have been rushed into use, despite data showing that these vaccines are neither safe nor effective.
With the almost certain probability of serious adverse effects, as described by researchers at the Salk Institute, after getting the JAB, many vaccinated patients now are regretting their choice to get these unapproved Jabs that have never been proven safe and not proved to be effective against the SARS-CoV-2 virus and its spread and transmission.
Prior COVID-19 infection but not ongoing Long-COVID-19 symptoms were associated with an increase in the risk of self-reported adverse events following BNT162b2/Pfizer vaccination.
Long-COVID-19 was defined as symptoms persisting >2 months to vaccination. What this means, simply is, that if you have been exposed to the SARS-CoV-2 virus that causes COVID-19, you are at increased risk of experiencing an adverse reaction or event after getting the vaccine. Those who had experienced persistent COVID-19 symptoms greater than two months before getting the vaccine did not experience the adverse events, but it is now clear, these people do not need the vaccine, and studies reveal that natural immunity is better than the immunity one gets after the vaccine.
The simple answer is, No, you do not need to get vaccinated if you have already experienced any symptoms of COVID-19. You are already immune to the virus, and many people are at increased risk of adverse events, and should not get the vaccine.
COVID19 Vaccine Safety and Effectiveness
Main concerns regarding Viral vector vaccines for the SARS-CoV-2 virus.
Phase 3 Trials Usually take Years before a Vaccine is FDA Approved
Many people are concerned, “How these vaccines are messing with your genes or genetic material”
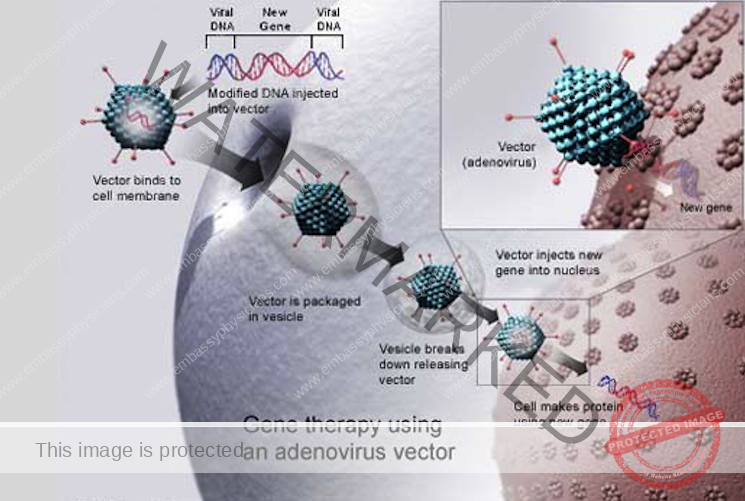
Gene therapy is not a new field; it has been evolving for decades. Despite the best efforts of researchers around the world, however, gene therapy has seen only limited success.
Why?
Gene therapy poses one of the greatest technical challenges in modern medicine. It is very hard to introduce new genes or genetic material into cells of the body and keep them working.
These COVID19 vaccines are injected IM or intramuscular into your arm, with the intent of these viruses to infect these muscle cells only.

One concern is the question of which cells are infected with these vaccines. Traditional vaccines work by introducing a dead or inactive pathogen into your body in order to stimulate the immune system into developing a immune response – antibodies, so that if you get infected with the live dangerous pathogen later, your bodies immune response is already set to fight the pathogen, allowing to survive the infection without getting sick or dying.

But viral vector vaccines work by introducing or “transfecting” foreign genetic material by infecting your own bodies cells with the intent of having these infected cells incorporate a foreign protein marker into your bodies healthy cells membranes. This is done to insure that your bodies immune system can be introduced to these foreign proteins that are found on the bad viruses, in this case, the SARS-CoV-2 virus, and then be able to develop antibodies to the SARS-CoV-2 virus when it infects your body at a later date.

Johnson & Johnson
One of the difficulties with transfection is introducing changes into the wrong cells could cause health problems for the patient. Simply injecting into the arm cannot keep these viruses from circulating around the body and infecting other cells, that may cause serious health risks, morbidity, and mortality.

Moderna and Pfizer-BioNTech Vaccines
For example, improper targeting could incorporate the genetic material into a patient’s germline, or reproductive cells, which ultimately produce sperm and eggs. Do we know what the long term effects might be if the vaccine infect cells located within your nervous system or spinal cord? Could this result in seizure like activity or paralysis?
Also, past research has shown that there can be serious health risks whenever receiving viral vector injections.
Our immune systems are very good at fighting off intruders such as bacteria and viruses. Viral vector vaccines must also be able to avoid the body’s natural surveillance system.

An unwelcome immune response could cause serious illness or even death. Both the Pfizer-BoiNtech and the Moderna vaccines use lipid nano-particles to encapsulate the mRNA so that the genetic material can be injected into your muscle tissue with the desired result of having these lipid nano-particles coming into contact with your cells membranes, then having these lipid nano-particles merging with your cells membrane and this resulting in the foreign genetic mRNA being infected or introduced into your arms muscle cells.

Then the mRNA essentially hijacks your cells protein synthesis machines, and your infected “vaccinated” cells start to make the spike protein that is eventually incorporated into the infected cells membrane to stimulate your bodies immune response to produce antibodies against the SARS-CoV-2 virus.
If the lipid nano-particles break down before they can merge with your cells membranes, the exposed mRNA can elicit a severe anaphylactic reaction inside your body and can result in death.

Our bodies immune response can react to such viral vectors for reasons we are not entirely sure of.

Jesse Gelsinger
The story of Jesse Gelsinger illustrates this challenge. Gelsinger, who had a rare liver disorder, participated in a 1999 gene therapy trial. He died of complications from an inflammatory response shortly after receiving a dose of experimental adenovirus vector. His death halted all gene therapy trials in the United States for a time, sparking a much-needed discussion on how best to regulate experimental trials and report health problems in volunteer patients. Researchers attempt to use the lowest dose of virus that is effective, and whenever possible, they use vectors that are less likely to trigger an immune response.
What about the disrupting normal genetic activity in the hosts infected cells that received the viral vectors new and foreign genetic material?

A good vaccine therapy is one that will last. Ideally, introduced genetic material will continue working for the rest of the patient’s life. How do we insure that the introduced genetic material does not become a permanent part of the target cell’s genome, usually by integrating, or “stitching” itself, into the cell’s own DNA, and what happens if the gene stitches itself into an inappropriate location, disrupting another gene?
This happened in two gene therapy trials aimed at treating children with X-linked Severe Combined Immune Deficiency (SCID). People with this disorder have virtually no immune protection against bacteria and viruses. To escape infections and illness, they must live in a completely germ-free environment.
Between 1999 and 2006, researchers tested a gene therapy treatment that would restore the function of a crucial gene, gamma c, in cells of the immune system. The treatment appeared very successful, restoring immune function to most of the children who received it.

But later, 5 of the children developed leukemia, a blood cancer. Researchers found that the newly transferred gamma c gene had stitched itself into a gene that normally helps regulate the rate at which cells divide. As a result, the cells began to divide out of control, causing leukemia. Doctors treated 4 of the patients successfully with chemotherapy, but the fifth died.
Newer viral vectors have features that target DNA integration to specific “safe” places in the genome where it shouldn’t cause problems. But shouldn’t long term studies be demanded to insure these complications will not be occurring with these COVID19 viral vector vaccines?
Another concern deals with the fact that everyone of these viral vector vaccines attempts to stimulate the hosts cellular and humoral immunity by incorporating a specific spike protein from the coronavirus into the infected host cells of the person getting the vaccine. Since this spike protein is foreign to the host and your own bodies tissue markers, the only way it can elicit an immune response, is that it has to recognize this new protein as foreign.

In so doing so, however, when this happens, how do we know for certain that the bodies own immune response won’t at some point down the line, start attacking these cells as being “bad cells” – in the same way they would necessarily attack the foreign viral particles with the same protein spikes you now have on your own cell membranes; resulting in an auto-immune illness whereby the body attacks these very same cells that were only intended to stimulate the bodies immune responses when and if it were infected with the virus sometime in the future?
And if we cannot be certain which cells, the viral vector vaccines will infect and incorporate the virus spike proteins, how can we be sure our bodies will not start to attack cells in our bodies, other than the muscle cells in our arm? Again, what if the vaccine infected brain cells, spinal cells, cardiac tissue cells, liver cells, pancreas cells? Would these organs suffer from the transfection of the viral material over many months or years?

Would our immune cells then start to attack these transfected cells and organs throughout our body and result with diseases like diabetes, cardiac failure, kidney failure, paralysis, rheumatoid arthritis, and Alzheimer’s, just to name a few?

The problem is, no long term studies were done and completed to determine the long term effectiveness and safety of these new viral vector vaccines. So we simply do not know what may happen. There is no way to say that these complications will even happen, perhaps these will never occur. But as these vaccines were delivered under emergency use authorization, the requisite long term safety and effectiveness studies were not done. Consequently we cannot say that any of the for mentioned adverse events will not happen; we can only know his with the appropriate long term studies.

Mild Illness
It is apparently becoming more evident that the SARS-CoV-2 virus is both: not as deadly as we once thought, and we now know, that we have good pharmaceutical therapy to safely manage and treat COVID19 in those patients who may contract the disease after being infected with SARS-CoV-2 virus. Furthermore, most people who get infected with the SARS-CoV-2 virus, will never know they were, and most of them will suffer a mild cold-like illness at worst.

Ebola Outbreak
So, are the potential risks and problems that maybe associated with receiving the viral vector vaccines insignificant enough to outweigh the risks of an infection with the SARS-CoV-2 virus? I would think a virus like Ebola that would most certainly kill you even with treatment is one pathogen that a virus vector vaccine would be beneficial, as the risks of the vaccine are insignificant when compared to the high mortality rates observed with the Ebola virus. But these has not shown to be the case with the SARS-CoV-2 virus.

Another important concern about these vaccines is efficacy, especially long term, what good is a vaccine if it only last a few months?
RNA viruses evolve quickly
The genetic material of all viruses is encoded in either DNA or RNA; one interesting feature of RNA viruses is that the change much more rapidly than DNA viruses. Every time they make a copy of their genes, they make one or a few mistakes. This is expected to occur many times within the body of an individual who is infected with COVID-19.

This means that if you do get the vaccine, and even if it is effective against the viral strain it was intended for, it may be completely ineffective against later strains that will appear in nature and in your body. So the vaccine is essentially useless, unless you get a new vaccine for each mutation. This is the reason the scientific community has not been able to develop an effective long term vaccine for the HIV virus, another RNA virus that mutates very quickly.

At the time of this writing three vaccines have been in use within the US. There are reports of adverse events, deaths, and many people are for the vaccines, and there are many arguing for the need for further studies and are warning people not to get the vaccines. Many tech giants are censuring or de-platforming anyone who comes out arguing for caution and refrain from these products until the requisite and appropriate studies be performed before accepting these pharmaceuticals as safe and effective.

There are many videos online revealing people with chronic movement disorders, tremors, neurological disorders, allergic reactions, and many sporadic reports of death and other serious adverse events.

The online vaccine adverse event reporting website, VAERS, has been up and running for years. You can research for the number of any specific adverse event such as death, for any vaccines, in any state, and by manufacturer and lot number, just to name a few.
Total US Deaths by Time Interval from Vaccination
80% of all Deaths Occur Within the First Two Weeks
Reported on 3/26/2021

United States Department of Health and Human Services (DHHS), Public Health Service (PHS), Centers for Disease Control (CDC) / Food and Drug Administration (FDA), Vaccine Adverse Event Reporting System (VAERS) 1990 – 3/26/2021, CDC WONDER On-line Database. Accessed at http://wonder.cdc.gov/vaers.html on Apr 7, 2021 4:06:25 PM
Note that these do not include deaths around the world.
There is a problem with analyzing COVID19 vaccine adverse events: They are not included in the Table of Reportable events as required by law – so reporting is voluntary, unless required by the Vaccine Manufacturer. Plus, they only account for events in the US. Subsequently, If you carefully tally the reported deaths from around the world, you will learn that the death rate from the SARS-CoV-2 virus vaccines is grossly under-reported.
An Evidence Review from the Penn Medicine Center for Evidence-based Practice revealed Severe systemic adverse events were reported by as many as 10% of trial subjects, prior to EUA release. For a disease that virtually has almost a 100% survival rate with prompt and effective treatment, a rate of 10% for serious events which includes death, does not appear to balance the risk of use of the vaccines.
The Penn Study concluded that there is not sufficient evidence to support any conclusions on the comparative safety of different mRNA vaccines; meaning, longer term studies are required.


The other shots approved in Europe, developed by Pfizer and Moderna, have been linked to similar temporary side-effects, including fever and fatigue.
But with the AstraZeneca shot the latest to be rolled out, health authorities in France have issued guidance to stagger giving the shot, two regions in Sweden paused vaccinations, and in Germany some essential workers are refusing it.
If you look back and review the press regarding the Hong Kong Flu back in 1968-69, you will see almost an identical frenzy and controversy surrounding the pushing of the vaccine they deemed as necessary and in the end, fewer than about 50% of the population chose to get the vaccine, which by the way, was not an experimental viral vector vaccine.
No one is sure how many deaths and adverse events are considered acceptable, but if it is you that experiences the adverse event, nothing else really matters; especially since, as more experts are realizing the survival rate of COVID19 is nearly 100% with prompt and effective treatment.

You can fool all the people some of the time, and some of the people all the time, but you cannot fool all the people all the time.
Abraham Lincoln
Addendum
Our Federal Government has Financial Stake through BARDA, NIAID, and OWS (Operation Warp Speed of Department of Defense) in two of the COVID19 Vaccines released for use by Emergency Use Authorization:

Moderna COVID‑19 Vaccine (mRNA-1273)
Produced in US
Authorized for use Canada, EU, Faroe Islands, Greenland, Iceland, Israel, Liechtenstein, Norway, Qatar, Saint Vincent and the Grenadines, Singapore, Switzerland, United Kingdom, United States.
This Company also received $5,896,492,979.00.
Financial Associations: Moderna, BARDA, NIAID

COVID-19 Vaccine AstraZeneca Adenovirus Vaccine
Covishield
Produced in UK
Authorized for use in Argentina, Bahrain, Bangladesh, Barbados, Brazil, Chile, Dominican Republic, Ecuador, El Salvador, Egypt, EU, Guyana, Hungary, India, Iraq, Maldives, Mauritius, Mexico, Morocco, Myanmar, Nepal, Nigeria, Pakistan, Philippines, Saint Vincent and the Grenadines, South Africa, South Korea, Sri Lanka, Taiwan, Thailand, UK, Vietnam
This Company also received Federal Funding of $509,650,000.00.
Financial Associations: OWS, BARDA
The US Federal Associations
BARDA

The Biomedical Advanced Research and Development Authority (BARDA) is a U.S. Department of Health and Human Services (HHS) office responsible for the procurement and development of medical countermeasures, principally against bioterrorism, including chemical, biological, radiological and nuclear (CBRN) threats, as well as pandemic influenza and emerging diseases.
https://www.phe.gov/about/barda/Pages/default.aspx
NIAID

NIAID conducts and supports basic and applied research to better understand, treat, and ultimately prevent infectious, immunologic, and allergic diseases. For more than 60 years, NIAID research has led to new therapies, vaccines, diagnostic tests, and other technologies that have improved the health of millions of people in the United States and around the world. NIAID is one of the 27 Institutes and Centers of the National Institutes of Health (NIH).

https://www.niaid.nih.gov/about/niaid-organization
OWS

OWS, Operation Warp Speed, is an unprecedented leap toward a historic breakthrough that will save countless lives. It is leveraging the best experts from the federal government and private industry to develop effective vaccines and therapeutics quickly without compromising safety.
https://www.defense.gov/Explore/Spotlight/Coronavirus/Operation-Warp-Speed/